
Cessation
Summary
One of the four key goals the Wyoming Tobacco Prevention and Control Program (TPCP) shares with the federal tobacco prevention and control program is to increase tobacco quit attempts and successes (Centers for Disease Control and Prevention [CDC], 2015). Reductions in tobacco consumption resulting from utilization of tobacco cessation services will result in a decline in tobacco-related sickness and death.
The earlier in life tobacco users quit, the greater health and financial benefits they will experience (CDC, 2015). The percentage of Wyoming high school smokers trying to quit has been declining since 2001, as has the percentage of U.S. high school smokers trying to quit (Youth Risk Behavior Surveillance System [YRBSS], 2015).
The Wyoming Department of Health sponsors the Wyoming Quit Tobacco Program (WQTP) to help Wyoming tobacco users quit. Since first offering services in 2013, National Jewish Health has helped 30% of enrollees quit (WYSAC, 2018b). Most WQTP enrollees say the primary way they learn about the WQTP is through a healthcare professional, suggesting that WQTP enrollment could be increased through additional collaboration with healthcare professionals. WQTP participants who use coaching and medication are the most likely to be successful in quitting.
Tobacco Use in Wyoming
Tobacco use is relatively common among Wyoming youth and adults. Wyoming high school students tied for the third highest in the United States for smoking prevalence in 2015, with no statistically significant gender difference (YRBSS, 2015). The percentages of Wyoming and U.S. high school students who smoke declined between 1995 and 2015:
- The cigarette smoking rate among Wyoming high school students declined from 40% in 1995 to 16% in 2015 (WY YRBS, 2015).
- The U.S. high school smoking rate declined from 35% in 1995 to 11% in 2015 (YRBSS, 2015).
In 2017, the cigarette smoking rate among Wyoming adults was 19%, with no statistically significant gender difference. For comparison, the median for all states and territories was 17%. The smokeless tobacco use rate for Wyoming adults was 9%, much higher than the national median of 4%. Smokeless tobacco use in Wyoming has a statistically significant gender difference (Behavioral Risk Factor Surveillance System [BRFSS], 2017). In 2017
- The smokeless tobacco use rate among Wyoming men was 17%.
- The smokeless tobacco use rate among Wyoming women was 1%.
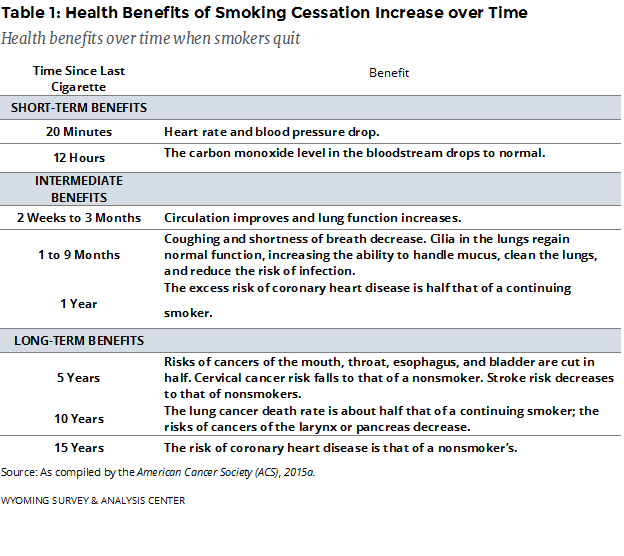
Health Benefits of Smoking Cessation
Evidence suggests that smoking cessation stops the processes which lead to cancer (CDC, 2010). Smoking cessation has various short- and long-term health benefits (Table 1). Some health effects of smoking cessation (e.g., increased lung functioning) are evident within a few weeks or months of quitting, suggesting that relatively brief periods of abstinence have health benefits. Others (e.g., reduced risk of stroke) are not fully evident for five years or longer, reflecting the benefits of long-term smoking cessation (as compiled by the American Cancer Society [ACS], 2015a).
Health Benefits of Smokeless Tobacco Cessation
Just as smoking cessation reduces the health risks associated with smoking, smokeless tobacco cessation reduces the risks associated with its use. These risks include the following (as compiled by the ACS, 2015b):
- Exposure to at least 30 cancer-causing agents, including those that cause cancers of the mouth, esophagus, and pancreas;
- Increased risk of coronary artery disease;
- Delayed healing of injuries and wounds;
- Gum recession resulting in bone loss and decay of exposed tooth roots; and
- Risk of having leukoplakia (lesions of soft tissue in the mouth that can become cancerous).
Quit Attempts by Youth in Wyoming
In 2015, the percentage of Wyoming high school smokers trying to quit was higher than the percentage of U.S. high school smokers trying to quit (YRBSS, 2015). Between 2001 and 2015, the percentage of Wyoming high school smokers who had tried to quit smoking cigarettes during the 12 months prior to being surveyed declined from 58% to 53%. Nationally, the percentage of high school smokers who tried to quit smoking cigarettes declined significantly from 57% in 2001 to 45% in 2015 (YRBSS, 2015).
Quit Attempts by Adults in Wyoming
In 2017, 87% of current adult smokers had made at least one 24-hour (or longer) quit attempt in their lifetime. Almost half (48%) of current smokers had made a 24-hour (or longer) quit attempt in the year prior to being surveyed. Neither of these are statistically significant increases since 2010 (WYSAC, 20108a).
Healthcare Professionals’ Role in Cessation
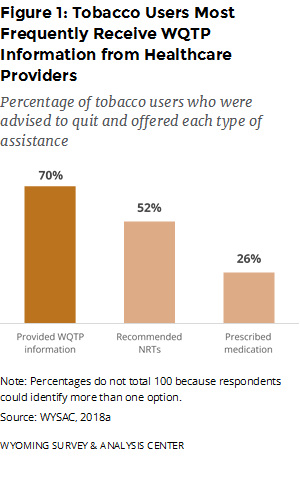
Healthcare professionals play a vital role in the Wyoming TPCP’s efforts to increase the number of individuals who quit using tobacco. Healthcare providers can screen their patients for tobacco use. Over half (55%) of current tobacco users who had seen a healthcare provider in the past year were advised by a health professional to quit using tobacco. This result has remained stable since 2010. This advice most often included information about the WQTP. Prescriptions for cessation medication were the least common form of assistance provided (Figure 1; WYSAC, 2018a).
The Wyoming Quit Tobacco Program (WQTP)
The WQTP assists Wyoming residents who want to quit using tobacco by offering them telephone-based cessation coaching and nicotine replacement therapies (NRTs) or prescription medications. On February 15, 2016, the WQTP began offering free Chantix (the most popular prescription medication) to enrollees. The WQTP requires enrollees to use phone coaching to order NRTs or be eligible for free Chantix.
WYSAC conducts monthly surveys of WQTP enrollees seven months after their enrollment for the Wyoming Department of Health, Public Health Division. The majority of people who enroll in the WQTP do so to get help quitting cigarettes, though some seek help quitting smokeless tobacco, ENDS, and/or other tobacco (e.g., cigars, cigarillos, little cigars, hookah, and pipes).
Phone coaching is often the most commonly used of the three major program components (phone coaching, NRTs, and prescription medications). Most enrollees used NRTs, which are mailed to enrollees’ homes for free.
National Jewish Health has been the WQTP service provider since 2013. Over that time, they have helped 30% of enrollees quit using tobacco, as defined by 30 days of abstinence from using tobacco products (not including vaping/electronic nicotine delivery devices) when interviewed seven months after enrollment (WYSAC, 2018b).
WQTP enrollees are a unique subpopulation of Wyoming tobacco users trying to quit. They are more likely to be successful in quitting than the broader population of Wyoming tobacco users. Based on the 2017 Wyoming Adult Tobacco Survey (ATS) data (WYSAC, 2018a) Wyoming cigarette smokers who made a recent quit attempt without using any cessation aids had a 16% success rate. The cumulative quit rate for National Jewish Health is 30% (WYSAC, 2018b), suggesting that WQTP enrollees are 1.9 times more likely to quit than Wyoming smokers who made a recent quit attempt without using cessation aids. Using WQTP components (such as coaching, Chantix, or NRT) greatly increases enrollees’ chances of quitting. Enrollees who use coaching and medication often see the greatest success rates. The requirement to complete coaching to obtain medication makes it difficult to tell which of these components is the primary contributor to this success.
References
American Cancer Society. (2015a). Benefits of quitting smoking over time. Retrieved April 18, 2016, from http://www.cancer.org/healthy/stayawayfromtobacco/benefits-of-quitting-smoking-over-time.
American Cancer Society. (2015b). Health risks of smokeless tobacco. Retrieved April 19, 2016, from http://www.cancer.org/cancer/cancercauses/tobaccocancer/smokeless-tobacco.
Behavioral Risk Factor Surveillance System [Interactive Database 1994-2017]. (2017). Atlanta, GA: Centers for Disease Control and Prevention. Retrieved November 27, 2018, from https://www.cdc.gov/brfss/brfssprevalence.
Centers for Disease Control and Prevention. (2010). How tobacco smoke causes disease: The biology and behavioral basis for smoking-attributable disease–2010. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
Centers for Disease Control and Prevention. (2015). Promoting quitting among adults and young people: Outcome indicators for comprehensive tobacco control programs—2015. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
WYSAC. (2018a). 2017 Wyoming Adult Tobacco Survey [Data file]. Laramie, WY: Wyoming Survey & Analysis Center, University of Wyoming.
WYSAC. (2018b). Wyoming Quit Tobacco Program Follow-Up Survey: January – June 2018 interviews by M. Kato, T. C. Cook, L. H. Despain, & J. R. Simpson.. Laramie, WY: Wyoming Survey & Analysis Center, University of Wyoming.
Youth Risk Behavior Surveillance System [Data File 1991–2015]. (2015). Atlanta, GA: Centers for Disease Control and Prevention. Retrieved June 12, 2014, from http://www.cdc.gov /healthyyouth/yrbs/index.htm.
